

Turn on the Thinking Cap
Update on 6/24/2021: Women are finding this article to be extremely useful. Please read this article fully. Evaluate the list of genetic variations and order genetic testing with your healthcare professional. It’s not just about MTHFR. There are more to evaluate. Details below.
UPDATE on 2/13/2012: This is no longer a theory as current research supports it. This research has yet to be published. First, read my theory below and then I will provide the proof.
This theory is born out of wondering why some women are experiencing recurrent pregnancy loss, have had all sorts of laboratory and physical tests done yet the only thing that shows up is a heterozygous A1298C MTHFR mutation OR a heterozygous C677T mutation along with a normal homocysteine level.
What do women typically hear as recommendations when having heterozygous MTHFR mutations along with normal homocysteine levels?
We don’t see risk associated with heterozygous MTHFR mutations when homocysteine levels are fine. Heterozygous A1298C (or C677T) is a mild and common mutation seen in the population. No treatment is necessary.
Researchers, geneticists and doctors do not appear to be considering the fact that a developing baby is made from two sets of genes:
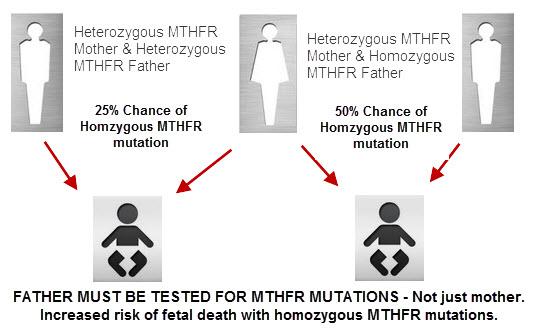
The Mother’s AND The Father’s MTHFR Genes and the Odds of Inheritance:
 Explanation:
Explanation:
If the mother is heterozygous A1298C and the husband is also carrying a heterozygous A1298C mutation – then the likelihood of baby having two copies of A1298C mutations exists.
In fact, the likelihood is at least 25% that baby can be homozygous A1298C.
Let’s look at another scenario:
Mother has a heterozygous A1298C mutation and the father has a heterozygous C677T mutation.
The likelihood that the developing baby has a compound heterozygous mutation is at least a 25% reality.
Compound heterozygous MTHFR mutation is also not great to have as the MTHFR mutation has significantly reduced function. The function of the MTHFR gene is at 50% capacity when one has a heterozygous A1298C mutation and a heterozygous C677T mutation.
I’m not going to begin explaining the reality of a homozygous A1298C or homozygous C677T father.
Research does state this:
…combined MTHFR mutations likely carry a selective disadvantage and contribute to decreased fetal viability, especially during times of folate insufficiency…. This study provides evidence that the combined effects of multiple mutations on phenotype, particularly in the case of common polymorphisms, are not restricted to intergenic interactions. The recognition that combined MTHFR genotypes may influence pregnancy outcomes further demonstrates both the clinical significance of this gene and the potential protective role of folate sufficiency.[1]
That said, it is best to proactively treat for MTHFR mutations in all its forms because the baby may carry more than just the mother’s MTHFR mutation – but the father’s MTHFR mutation as well.
Doctors must test the future father’s genes for MTHFR mutations and understand the potential risk to developing baby. Then take the necessary precautions for the woman (and baby) by supplementing or prescribing properly.
Doesn’t this explain why so many women with heterozygous MTHFR mutations still miscarry – at least in part?
Obviously there can be other causes here as well for miscarriage – but let’s keep it focused to MTHFR.
How to address MTHFR mutations and pregnancy:
- Future mother and father: Get an MTHFR genetic test plus identify important genetic variations such as COMT, GST, GPX, MTHFD1, DHFR and over 100 others in a comprehensive 100+ page report.
- Future mother: Get tested for MMA, S-adenosylhomocysteine and homocysteine (only focusing on MTHFR here. Obviously other testing and physicals need to be done).
- Take appropriate action to ensure a safer pregnancy.
UPDATE on 2/13/2012: I found the research and it is not yet even published – it is that new.
Results of the study:
The overall, heterozygous and/or homozygous point mutations in FVL – FVR2, ApoE2, PAI-1, MTHFR C677T – A1298C, and ACE genes were associated with recurrent pregnancy loss (RPL). There was no meaningful association between RPL and other studied genes.
Current results showed that RPL is related to combined parental (not only maternal) thrombophilic gene mutations. [2]
Take-Home Message:
If you have recurrent pregnancy loss or are considering becoming pregnant, then I highly recommend you ask your doctor to test you AND your partner for the genes:
- FVL – FVL2
- ApoE2
- PAI-1
- ACE
- MTHFR
The research by Ozdemir proves the point that genetics from the father and mother must be considered in recurrent pregnancy loss.
Whether heterozygous MTHFR by itself causes recurrent pregnancy loss is still to be debated; however, when combined with the above mutations, the effect is clear.
I need you to Tweet, Share, Like, Email, Print, Post on Forums – do everything you can think of to get this article in the hands of those who need to read it.
This article can save the lives of babies every year. Add the ability to help potential parents avoid the devastating loss of their baby.
Health care needs to be more aware of prevention. This is a classic example of why.
Read this article on MTHFR and Pregnancy to optimize your pregnancy and your future child!
Resources:
[1] Isatolo et al, Neonatal and Fetal Methylenetetrahydrofolate Reductase Genetic Polymorphisms: An Examination of C677T and A1298C Mutations, American Journal of Human Genetics
[2] Ozdemir et al, Recurrent Pregnancy Loss and Its Relation to Combined Parental Thrombophilic Gene Mutations, Genetic Testing and Molecular Biomarkers
Hi Dr. Ben! After 4 miscarriages and one anencephalic(twin) my other twin is healthy. I decided to get tested for mthfr. I am heterozygous for c677t. I have always had low progesterone as well. With my twins I was on a suppository of progesterone from week 3-14. I am scared to attempt another pregnancy but want to desperately have one more child. I’ve heard that this mutation can cause down syndrome and other NTDs? If I take methyl folate and methyl b12 will that lower my odds ? I’m meeting with a maternal fetal medicine doctor in a week. I have no family history of downs or anencephaly besides my own anencephalic child. Please help! Thanks so much.
Interesting. Thank you.
I am homozygous for 03 P39P and A1298C.
My oldest daughter is hetero for C677T, 03 P39P and A1298C.
After her I had at least 4 miscarriages before successfully having her younger sister. Have not tested her younger sister yet, but at least she will be hetero for 03 P39P and A1298C.
Father has not been tested yet. We are trying for 1 more, but have had several more suspected miscarriages already. Am focusing on the supplements now, aspirin and low dose steroid during first half of cycle and progesterone support after as well as being as healthy as I can.
At least I have hope knowing that I just need to ‘wait’ for the baby with the viable genes…. and we’ve got 2 girls who are doing great from this waiting game…
My husband and I have been trying to conceive for over a year. I have had 3 miscarriages and finally changed doctors and he has ordered a slew of lab work. It came back that I am a compound carrier of both those MTHFR mutations. My homocysteine levels are normal as well. All labs ordered were normal except this one and my thyroxine. Hopefully this is my issue and it can now be address. I’m sure my age plays a role as I am 37 and trying to concieve for the first time in my life.
I have had 7 miscarriages(2 2nd trimester) and 3 live births. I was tested and am hetero C677T, homocysteine normal. The OB says this is not a contributing factor to m/c. My husband was just tested and is hetero C677T and FVL Ii hetero(A20210G). His B12 was very low. Can you please advise on whether that makes us more prone to m/c? Also, is there something we should do should do if we get pregnant again to increase our odds of a healthy baby and full pregnancy?
Is this research still going?
I’m adopted so I have no idea what my parents were.
I was a big 8lbs baby, my mother was O- for blood type.
I’ve had four, 1st trimester, miscarriages. And lost five babies.
On my 3rd miscarriage they said I had mthfr and left it at that.
I now just found out today that I have homozygous a1298c
But I have gone almost my whole pregnancy without treatment. I am 39 weeks and have just started taking lovenox generic, once daily 40mg sq
They say I’m at higher risk for having blood clots.
Also noticed in the pregnancy, baby is the 15% of growth, and my uterus measures 34 weeks even though I’m 39. They say it’s constricting the baby from growing.
Hi Dr. Ben
I’m not quite sure where to start, I’m 28 yrs old and recently married. Me and my husband just suffered our first loss together, however I’ve had 6 other losses. All my pregnancies seem to end about the same time:6w, except for one, I had a little girl in 2008 but she had IUGR and stopped growing at 22w in the womb, died at 8 days old. We just found out I’m heterozygous c677t, but blood clotting tests are showing everything’s fine. I’ve been treated with both baby aspirin and heparin for two pregnancies,and progesterone in another, all ended up mc’s. I’m wondering if my c677t could be so deficient in folic acid to be causing this? I know I need to take Methylfolate and not folic acid now, didn’t know that before. Anyway, I have almost all of the symptoms of my mutation, so maybe? I just dnt know what else to look for, and my pregnancies have not been with the same man. My doctor wants to karotype me, but I don’t feel that’s the problem solely on my daughter. I so far, have no living children and I’m terrified of having another loss. My current doctor said there’s nothing that can be done at this point,besides keep trying till we have a baby that sticks. This scares me as I don’t want to be a woman with 20 some mc’s. I’ve been researching a lot since my last loss around Mother’s Day, of all days, my homocysteine was not checked, she said it wasn’t necessary as Heter c677t wouldn’t be causing my losses. Please help me figure this out, I have an appt with my first RE next month, but I’m still scared. Thank you
[…] mutation. This is a great article from MTHFR.net about how a dad's MTHFR status is important too: Heterozygous A1298C OR Heterozygous C677T MTHFR Mutation and Recurrent Pregnancy Loss? Consider This… Adoring our gorgeous (2007) and (2013) Missing (2006) and (2012) *Might* be TTC a 3rd […]
Hello Dr I have c677t mutation and A1298c mutation . What can I do to get pregnant ? Every time I get pregnant it ends in mc at round 5 to 6 weeks and I’ve had 7 in 2 years still no baby 🙁 my Dr had me take folic acid 4mg daily and a baby aspirin but so far nothing.
You might try a supplement with methylfolate (not folic acid) and methylcobalamin. I have both as well and kept miscarrying until I took these.
My N.D just discovered that I have MTHFR and am Heterozygous. I am 26 and have had 5 miscarriages, one early birth, and one living child of six years old. I have been through heavy metal poisoning, mold toxicity and severe chronic inflammations of the lymphatic system, it is really a miracle I am still alive. I am very excited, yes I said excited, to do research about this Genetic mutation and learn all I can. I have been through a lot and am hoping to find some answers. Thank you for being such a great resource and support of those suffering from this and seeking answers. I wish there was some thing more I could do to bring more understanding of MTHFR. Very grateful of your work, Joie
My story is that I had 2 children with no issues at all, and then 1 miscarriage, followed by another healthy pregnancy full term birth 5 months later. Something happened… and then I miscarried 4 times in a row, one of which was a second trimester loss and no reason was detected. I suspected a clot of some kind as that might not have been found. I saw an RE who did a full thrombosis panel on me and discovered Compound Heterozygous MTHFR as the only issue. His response was to give me folgard.. nothing else. I tried it his way and I miscarried a 6th time (5th in a row). Then I felt compelled do to my research and I found your site and information from Dr. Rawlins and began to see that folgard was a bad idea. My RE refused to listen even when I tried to explain. I think a lot of good doctors are just too stubborn to listen to what new information there is in this field, and it’s developing so rapidly. I discovered Methylfolate and began taking 3.75mg of Methylfolate + Methylcobalamin combined sublingually, and trying to modify my diet to limit my exposure to regular folic acid. I refused to take prenatals with folic acid in them. This time, I carried my baby full term and she was born with no abnormalities at all. I feel that this happened because of knowing what my body needed. I don’t yet know what my husband’s DNA holds, or any of my children, nor do I know beyond the MTHFR compound Hetero polymorphism. I’m not even sure where to go to get this testing done because so many doctors look at me like I’m sprouting a tail when I bring this up. I didn’t just have a healthy baby finally… My depression is GONE, my chronic fatigue issues are GONE, my memory is back, and my neurological problems are now GONE. I live in Utah… but have no idea where I can go to seek more information and help.
Hi there,
I am compound heterozygous for both the A&C MTHFR genes. i am 24 years old and have had 2 missed miscarriages. After demanding further investigation following my 2nd miscarriage (in australia they wont test till you have had 3 or more) i found out about my mutation. My doctor prescribed high dose vitamin B6, B12 and very high folate (megafol 5mg) daily. after reading everything online it looks like high dose folate is NOT the way to go! looks like i will need to purchase different supplements online.. i cant find them anywhere in sydney! I am studying to be a naturopath/ nutritionist so already eat a grain, dairy and processed food free diet.. im just not sure exactly what i should be taking..?
my homocysteine level cam back ‘normal’ (8) so my OBGYN isnt worried.. he is just going to put me on low dose aspirin (cartia) when we fall pregnant next. i cant find any OBGYN with knowledge into MTHFR either for a second opinion.
help!?
Dr. Lynch,
Thank you for this compelling article. I am compound hetero and my husband is homo (677) & hetero (1298). We have had 2 miscarriages, 1 daughter and now another miscarriage. I am Wondering if we are bound to miscarry half the time if the fetus is compound homo or hetero homo, and have to play the odds OR is there something we can actually do about it? If my husband is methylated better will the sperm be more favorable genetically or if I am methylated better can I compensate for a genetically poor fetus mthfr combination? We are trying figure out what we are in for.
Hello,
I’m heterozygouse for c677t and a1298c. I’m currently 7 weeks pregnant and don’t want to lose this baby also. I have had 4 healthy kids, then had 5 miscarriages one after the other. All chromosome tests came back normal on all the fetuses. I lost all at 10 weeks and I know that’s when the placenta takes over. I believe that I had clots. That’s my only explanation, since the doctors don’t know the cause besides me having MTHFR. All others tests done on myself were normal. Also my mom has had multiple miscarriages, but inbetween and different gestations. I believe I got the MTHFR mutation from her. Currently i’m on Lovenox 40mg once a day, baby asprin, and progesterone 100mg bid. Should I be taking nattokinase as well or that is too much? Anything else I should do? Thanks
I lost my first pregnancy at 12 weeks, they said there was a sac but no baby. A year later I had my daughter, she is 19 now and healthy. I tried to get pregnant again for years, but didn’t until she was 15. The same thing happened, lost this one at 9 weeks. My hormone levels were so high they thought I was having twins, but when they did the ultrasound there was a sac but no baby. Last year I lost another one at 5 weeks. I just found out about my compound heterogeneous mutation last month. This makes sense, but makes me really sad that this could have been avoided.
I had my daughter in 6-16-09 than I miscarried on4-1-10 @14wks than another miscarriage in 6-30-11 @16weeks. Had my daughter on7-2-12 than miscarried 9-23-13 @20weeks than miscarried at 14wks on12-23-14
I have been tested my thyroid was 0.43
homocysteine levels was 12.1
and I am hetero C677T
THATS THE ONLY THING THAT haS SHOWN UP
but know I dont know what my protocol should be
if anything and doc doesnt think that any of these things caused my missed miscarriages
all babies was fine heard and seen all babies and there heartbeats than one day at regular ob appt no heartbeat no reason no answers I am terrified to get pregnant again please help thanks
Hi Samantha – I can understand that you would be terrified to get pregnant again–you’ve been through a lot. Dr. Ben’s mission is to prevent disease, and a large part of that starts before babies are even born. Please see the ‘Optimizing your Future Child’ protocol that has helped many women in situations like yours have healthy pregnancies and healthy babies: https://mthfr.net/prenatal-supplementation-optimizing-your-future-child/2012/01/20/
Wishing you all the best. Please keep us updated with how you are doing!
Dr. Aron
Hi! I’m 28 and suffered 2 chemical pregnancies and 1 miscarriage at 8 weeks after a healthy sonogram and heartbeat. This is all within one year. I had all the blood work done and only thing it came back with is mthfr heterozygous. Currently I am on prenatal vitamin which has methylfolat, 1mg of extra methalolate as folate,baby aspirin & Crinone progesterone starting 3 days after ovulation. My miscarriage that was at
8 weeks started with intense spotting and eventually I had a spontaneous abortion and bleed out… I just want to know if my regimen seems sufficient to help with future pregnancy?
Hi Keri – Helping women in your situation is one of Dr. Ben’s passions. He has an extensive post on Prenatal Supplementation that other women have had success with: https://mthfr.net/prenatal-supplementation-optimizing-your-future-child/2012/01/20/. Once you’ve had a chance to read through this, feel free to post your specific questions there for the community.
Please keep us updated on your progress!
Dr. Aron
Hello. I have been researching as much as possible and have gotten a lot of great information from your site. I have posted before, but to refresh: I have had 2 miscarriages within the last year, both around 6 weeks gestation. I have been diagnosed with MTHFR Hetero A1298C. I have only ever done one blood test checking homocysteine and it was in the normal range (was pregnant at the time, but lost the baby shortly after). My husband recently got tested and found he has the Mutation too, except he is Hetero C677T and he had elevated homocysteine. Can this effect blood clotting in the fetus or would it only be a concern if I had elevated Homocysteine? Also, I know the article states that both parents can be a factor, but I’m not sure of the protocol for trying again in the future. Do you think blood thinners would be needed since we both carry the mutated gene? Thank you for all the great info.
Hi, I was just wondering why it’s so important for the father to be tested as well, if the woman already knows she has MTHFR? If she knows about it and is dealing with it appropriately, why does it help to know if the father has a mutation as well? Is there some protocol the father has to follow as well?
I know this thread is old but I’m desperate for some insight! I have 3 healthy children and 6 miscarriages. Our last 3 were within the last year at 18 weeks, 13 weeks, and 13 1/2 weeks. I was on aspirin and progesterone with all 3. We even attempted heparin with my most recent pregnancy. I’ve been gluten & dairy free for 3 years. Taking methylfolate and methykcobalamin and avoiding folic acid. My doctor’s dismiss my MTHFR (homozygous 1298) as being relevant to my losses. I know hubby has at least one copy of 677 as our children our compound heterozygous. Is there anything we could be missing? We have decided to be done with childbearing but I need some peace. Can’t help but hope for a surprise pregnancy but don’t have anything to change in an effort to have a healthy pregnancy. Would love any insight!
Forgot to add that my homocysteine has always been normal and that all other testing has been normal. Still no known cause for our losses.
Kelly – So sorry to hear about your struggles with miscarriages. Please take a look at this article where Dr. Ben discusses his prenatal supplementation approach. This could give you some insight that you can apply to your situation.
I lost my daughter at 38 weeks (8 weeks ago). The cord was wrapped around her neck, but MD could not find reason for her death. I just got the blood results back saying that I am heterozygous for mthfr-c677t and homozygous for pai-1 (4g/4g). I also have a family history of thrombosis. My mother died from a PE a few years ago. Just wanted to know how the next pregnancy I should be treated? Thanks.
Jamie – So sorry to hear about your daughter. Based on your past medical history and family history, you may want to reach out to a physician in the Physician Directory for a consultation. You can also find more about Dr. Lynch’s general Prenatal Supplementation strategy here. Also check out this article for a better sense of MTHFR’s significance. I hope this helps. Please keep us updated on your progress.
Hi Dr Aron & Dr Ben,
I have been diagnosed with the mutation C677 Heterozygous. As I was diagnosed I also got pregnant and I am now 16 weeks into the pregnancy with a boy. I have gotten conflicting advice from my fertility specialist and my general OB about my medications.
My fertility doctor prescribed me baby aspirin 100 mg and Enoxalow 40mg (similar to Clexane ) for the whole pregnancy and also recommends me to continue 2 months after I give birth. My OB has prescribed me with folic acid and vitamin Bs, and suggested I could stop with the aspirin and the Enoxalow as of week 12, with the argument that I do not fall in the riskzone for having trombofilia/bloodclots (judging from my own and my families medical history), and that my placenta/fetus is now well enough implanted into my uterus.
I have no records of trombofilia in my family (just an uncle with stroke at the age of 60). My mother however took 7 years to get pregnant with me and had issues with her placenta detaching throughout the pregnancy, bleedings etc. She also lost a baby at 6 months and had numerous misscarriges in btw me and my sister. She was never diagnosed with any mutation issues – think “back then” the issue wasn’t known.
I myself have tried to get pregnant for 4 years, and only now in July we were successful for the first time. I have had 1 known misscarriage in 2012 at week 6. In December 2014 I was operated for Endometriosis, and it was partly successfully removed.
Could you please give me some advise as whether to continue with Enoxalow and aspirin or not? Also, my sister is trying to get pregnant, what are the chances that she has the same mutation as me?
Thank you in advance.
Kind regards,
Hermine
I am C677T (homozygous), I also have SOD 2 (homozygous) and COMPT (homozygous) and had 2 healthy pregnancies at age 38 and 40. (Miracle?) I didn’t take any folic acid or B12 (Here in Europe – the netherlands – food isn’t fortified with it either) I was a stress-free vegetarian (low methionine diet) but did eat wheat and dairy. I did suffer from severe headaches though (more like herxaimer reactions) around my periods. I still do.
Followed by 6 miscarriages at age 43-44 at week 5 (3x), 8, 11 and 8). I was eating fish again – but no wheat, no dairy. At that stage and was not ‘stress-free’ anymore. (2 kids and a full-on business).
I also had 7(!) mercury fillings removed before at 43.
I’m 29 years old i have compound heterozygous MTHFR mutation , i discovered that after miscarriage at 12 week from a year . from that time i take B Complex Plus -Pure encapsulation by myself without doctor supervision after read many article about my case as there is no local methyl folate products in my country so I had to export it and i took it once daily ,actually i improved after that.
but now i discovered that i’m pregnant at about 6 week i didn’t know that and i made x-ray on respiratory tract when i was at 4 week , i don’t know if it will affect my pregnancy or not ?and i stopped my medication ( B Complex Plus -Pure encapsulation ) as i’m not sure about its safety during pregnancy i need your advice about what i should do and what i should take in my case
now i suffer form nausea ,feel uncomfortable , headache ,depression and general weakness ,loss of power
i don’t know if it due to pregnancy or due to stopping the methyl folate medication
sometimes i feel tendency to loss pregnancy I’m worried about any mental or congenital disorders may occur to the baby, i need some way to discover that early
I’m hoping that you can help provide me with some guidance. I am 31 years old and have had 2 miscarriages in the past 12 months. One at 5 and half weeks and one at 7 and half weeks. I have been tested for everything under the sun and they only found hetero A1298c. My fertility doctor stated that this was probably not adversely affecting my pregnancies, but did prescribe me Vitamed One RX. (has 400mg folic acid and 600 mcg as ((6S)-5-methyltetrahydrofolic acid, glucosamine salt) The website for it is https://www.vitamedmdrx.com/prenatal-vitamins/one-rx
I am thinking of finding a new doctor who has more knowledge about this, but am not sure what to ask them to look for and what things I should actually take. From what I’ve read I shouldn’t be taking that much folic acid. They haven’t tested my husband for MTHFR and haven’t indicated wanting to do so.
It’s super frustrating, but I’m convinced there has to be a reason for these miscarriages.
I would really appreciate any advice you can give. Thanks!
Heather – so sorry to hear about the miscarriages. Dr. Lynch discusses his general approach to prenatal supplementation in this article. The Physician Directory is a good place to start to look for someone who has completed some training with Dr. Lynch.
Hello Dr,
I am 24 years old and at 21 i had a thrombosis on my left leg. I am diagnosed with MTHFR C677T and A1298C heterozygous and also heterozygous with Factor V H1299R. My husband had a stroke at 20 years old. He was after that diagnosed with MTHFR C677T homozygous. We are trying for about a year to get pregnant without any luck. I have done my hormones analysis and also O.B. check-ups where everything is fine and functional. These days he is doing the spermogram and spermoculture. I am for the last 6 months on baby aspirind, B12 vitamin, Omega 3 and folic acid.
Could you please tell us what are our chances of getting pregnant or what else could we do in order to get pregnant and have a baby? I can go deeper into details if necessary, just tell me so.
Thanks,
Alexandra
Alexandra –
You and your husband – both – need to follow the recommendations here
https://mthfr.net/prenatal-supplementation-optimizing-your-future-child/2012/01/20/
You both need to supplement.
You may also need to take Lovenox or baby aspirin during pregnancy along with the recommendations above.
Do not take folic acid…here’s why
https://www.youtube.com/watch?v=cWFPRI6X7P4
Take natural folates – as discussed in the article link above – and they are found in those supplement recommendations!
Keep me posted! You’ll be surprised 🙂
Hi,
I just found out I have the C677T heterozygous and A1298C heterozygous after three consecutive miscarriages. I will start your prenatal vitamins ASAP. But my question is, what should we do if we test my husband and he too has one of these mutations? Does he too simply need to start active forms of methofolate or is there more he will need to do? And should we both be on them for 3 months before trying to conceive again? Thanks!
Hi Kari –
Yes you should both be taking prenatal support prior to conception – ideally.
We all should be taking active forms of folate – no matter if we have MTHFR or not.
Here is why – a great informative video which all should see –
https://www.youtube.com/watch?v=cWFPRI6X7P4
I truly recommend the Optimal Prenatal Protein Powder – vanilla. It’s so easy to make a smoothie in the morning – one for each of you. It is what I take each morning for breakfast – shhh 😉
Hi Dr!
I was hoping for some info in regards to pregnancy and heterozygous 1298. I had a miscarriage back in July 2015 that needed a D&C in August. From pathology testing, I was told it was caused because my baby had Down’s Syndrome. I was put on birth control in September after I had my first cycle, then in the beginning of October, I was in the hospital with a PE. The doctors there were convinced it was caused by the birth control I was put on due to the high amount of estrogen in it, but I think it was a combination of that, complications I had from the D&C and just not being active at all due to depression. I was put on blood thinners for 6 months. Well, fast forward to April of this year and my hematologist found that I had MTHFR heterozygous 1298, and I had also found out I was pregnant the week before that appointment. My doctor put me on Lovenox injections at 140ml a day. I had horrible reactions to the injections and stopped taking them and started taking baby aspirin instead, along with a slew of different vitamins for pregnancy. As of now, I’m just over 14 weeks along, everything is going well, and I feel great. My OB seems to think I’m a ticking time bomb by not taking the Lovenox injections and she wants me to see my hematologist, where they will most likely want me to take Heparin instead. I 100% do not feel comfortable injecting myself with unnecessary medications when I feel the PE I had was brought by the D&C and birth control, and I feel like the baby aspiring I’m taking is helping. I see the hematologist very soon, but what is the best course of action for me? Like I said above, I feel great! I’m much more active, eating well, and I’m actually losing weight even though I’m eating normally.
Thank you!
I just found out I am hetero c677t. I am 51 and had three normal pregnancies. My middle daughter who is now 22 years old is severely autistic, has epilepsy, OCD and polycystic ovaries. I was tested because I suffer severe depression and anxiety and have been through at least 10 anti-depressant prescriptions that have failed to do anything. Upon researching this after my appointment to find out exactly what I was dealing with, I have come to discover this can also cause insomnia, migraines, IBS, and joint problems all of which I have. I am also wondering if this has attributed to severe weight gain over the last ten years. At 40, I was 5’4″ and 105#’s, I was anorectic till I had my children and was able to maintain a normal weight after them. I have gained 85#’s in the last 10 years and am unable to take it off. I am also wondering if having my daughter tested would help her in anyway. I am at the beginning of this journey and trying to figure out a path to feeling better. I have always suffered from depression, anxiety, IBS and migraines. I remember being as young as 8 when the headaches and anxiety struck. They have prescribed an anti-depressant on my good list and I have just picked up the methofolate and the special B-12. So I am hoping for improvement. As for my daughter, is there a benefit to having her tested? Would it help prescribing seizure meds? I know there can be a benefit to the anti-anxiety meds and anti-depressant. We have been through many of those as well as a few anti-psychotics which we do not want to do again. We finally hit upon Zoloft, Buspirone and Clonopin as a combination that works pretty well. I am looking to help her feel comfortable in her own skin, sleep better and have a better treatment for her seizures as there has been an uptake in them this year. Before we only dealt with one or two a year, but this year she had one so severe she broke her front teeth, had severe gum damage and was knocked unconscious by it when she went face down onto a wood floor. Before she has always seem to have an aura and knew they were about to hit. This one hit her harder and quicker. Thank you for your time, I know this is a bit of a jumbled message. I saw that you said some of this could be autism related and wonder if this could be a source of autism. My other two children are adults and developed normally with no signs of being on the spectrum. My son has headaches and a sensitive bowel. He was diagnosed with ADD but his challenge there is an organizational one. Both my of my other kids are high achievers and are doing well outside of what I mentioned health wise about my son. We medicated his ADD for about 3 months, he did not like it and we chose to manage his behavior by working on coping mechanisms. At 20, he is doing well.
Hi Dr. Ben,
I have had 3 early miscarriages, all within 5 weeks. After almost 2 years of trying we finally decided to go to a fertility clinic and get help. I found out after the first 2 positive tests and having an RPL (recurrent pregnancy loss) blood work panel done that I am compound heterozygous for 1298 and 677. I am currently taking low dose aspirin, lovenox, progesterone, methly folate, methylcobalamin, I switched to an organic prenatal with folate (not folic acid), CoQ10, and the clinic put me on a low dose of prednisone to hopefully assist with inflammation. I am otherwise very healthy, eat well, have been trying to eat more healthy fat, oils, avocados etc as I am a vegetarian, and get a good amount of protein every day. I have also gotten my amalgams recently removed by a SMART certified dentist. Do you have any other suggestions? It is becoming very hard as it seems as soon as I get a confirmed blood work positive pregnancy test, I miscarry. Thank you for your dedication to raising awareness on this!
I am 1298cc homozygous, wild card. I have had 4 successful pregnancies. Just diagnosed so not sure where to start medication/supplement wise.
Hi
Very interesting. I am a heterozygous C677T woman and my husband is heterozygous C677T too. I have been pregnant 8 times. I have given birth to six children and have had two miscarriges. In two of my six children birth I had a placenta rupture late in the pregnancy, and one of my children died because of it. The daughter that survived the placenta rupture is homozygous C677T, which contribute to your theory. Unfortunate I do not know the genotype of my dead son, but some samples where kept and perhaps it is possible to obtain the genotype.
I also suffer from celiac disease, which was discovered late in life. It is common to have low B12 values in this condition, which again makes it more difficult to methylate.
These pages helped me understanding why my little baby son died.
Hi, you said, “DIAGRAM SHOWING INCREASED RISK TO FETUS FROM FATHER’S MTHFR MUTATION”, but I am not finding the diagram. Am I missing it somewhere?
Also, I am new to MTHFR, having heterozygous C677T. However, my son has heterozygous C677T and heterozygous A1298C. I believe that makes him a compound hetero. As far as I can tell, his father has to have the A1298C mutation, doesn’t he? Why is there an increased risk to the fetus if the father has MTHFR? Is the risk more so than if the mother has MTHFR? If so, why?
Thank you.