
Optimizing the health of unborn children is my passion.
I am pleased to state that January is named National Birth Defects Prevention Month by the National Birth Defects Prevention Network and the CDC. This month is broken down into four parts with each part focusing on a key component of birth defect prevention.
While I should be completely supportive of this fantastic cause, I am not. In fact, I am totally and utterly against one of their causes blended in with reducing birth defects.
Why?
Because it has to do with folic acid. My arch enemy. And it is also the arch enemy of unborn children – and children in general.
Folic Acid Awareness Week extends from January 5 – 11. Happily, I am extending the Folic Acid Awareness cause for years to come – only my cause is to establish folic acid as an anti-nutrient which is causing significant harm.
Yes, there are countless research papers out there which show that folic acid reduces neural tube defects. This is true. According to the Harvard Medical School:
In countries that require folic acid fortification, including the United States and Canada, the rate of neural tube defects has fallen by 25% to 50%.
After all, folic acid has no use biochemically in the body until it is converted into these other forms of folate such as:
- Tetrahydrofolate (THF)
- 5-formyltetrahydrofolate (Folinic acid)
- 5-10-methylenetetrahydrofolate
- 5-methyltetrahydrofolate (Methylfolate)
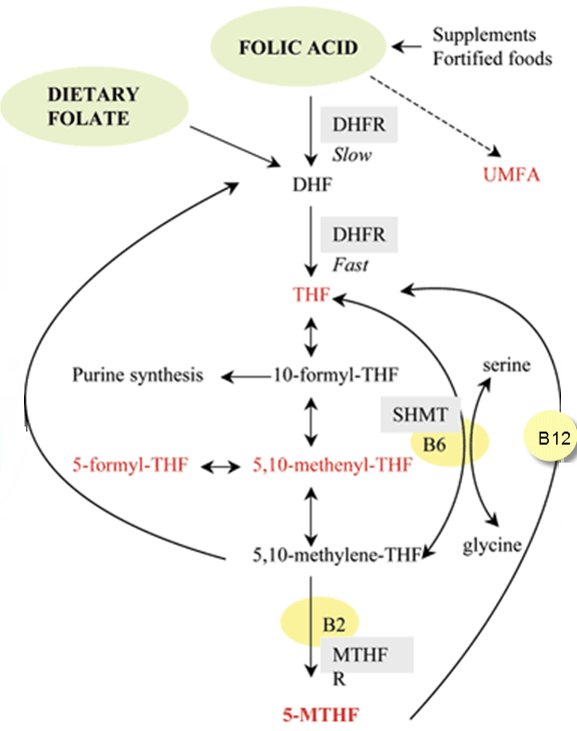
Let’s view how folic acid is changed into usable forms of folate by the body:
That appears to be a lot of work right?
It is.
And this is a very simplified outline of what it takes to convert folic acid into usable forms.
Imagine a mother – or child – or father – who has a problem in any one of these genes.
Then add on a potential deficiency of vitamin B12 (which is fairly common and often goes undiagnosed for years).
What happens is far from good.
You see the ‘Folic Acid’ moving to ‘DHF’ in the diagram above? Note how it states this is a ‘slow’ process?
Now note the dashed black arrow moving from ‘Folic Acid’ to ‘UMFA’
What is ‘UMFA’?
UMFA is the sound your body makes when you ingest too much folic acid. ‘Ummph’ It hurts.
Truly? UMFA = unmetabolized folic acid
What does that mean?
It means folic acid didn’t get processed by the body into usable forms of folate so your blood just has this synthetic nutrient floating around in it.
Is that ok?
According to researchers Obeid and Hermann:
Evidence of a negative health effect of free folic acid (FA) in blood is not consistent and suggests rather artificial factors. FA has no known cofactor function that would increase the likelihood of a causal role for free FA in disease development.
This means that since folic acid is totally synthetic, it doesn’t do anything to the body’s enzymes thereby rendering it harmless.
Let’s look at a compound which is a known killer: Carbon Monoxide.
How does carbon monoxide kill? Carbon monoxide kills because it preferentially binds to your hemoglobin 210 times stronger than oxygen which means your hemoglobin cannot bind oxygen well in the presence of carbon monoxide. The higher the levels of carbon monoxide, the less oxygen is bound to your hemoglobin causing decreased oxygenation and cell death.
Does folic acid do the same thing?
Yes, if you examine how folic acid binds to folate binding proteins (these carry folate around your body, the developing baby and breast milk) and folate receptors (these pull folate inside the cell and out of the blood) in the human body. Folic acid binds preferentially to folate binding proteins and folate receptors. This means that the folate binding proteins and folate receptors in your body, which are intended to bind methylfolate or folinic acid, are more likely to bind to synthetic folic acid.
The Annual Review of Nutrition published an article in 1990 states, “A major class, the high-affinity folate-binding proteins, show a preferential and tight binding of folic acid relative to reduced folates . . . Soluble forms of the high-affinity binders are present in serum and [breast]milk. [Folate binding proteins] serve to accumulate and stabilize reduced-folate compounds in milk and they may also facilitate the absorption of folates by the intestinal mucosa of neonates.”
If high-affinity folate binding proteins are bound to synthetic and inactive folic acid, what benefit is there to the developing baby? In fact, it would make sense that harm would occur as reduced folates are needed for DNA production, balance methylation and support neurological development.
How can reduced folates get into the intestinal mucosa of the baby if they are not bound to the folate binding proteins? Are we setting up our new generation with weakened intestinal linings? Food allergies are definitely on the rise.
Autism is definitely on the rise and we all know those with autism have significant gut issues.
We know that synthetic folic acid reduces the incidence of neural tube defects. What about if we used methylfolate instead? Can methylfolate reduce the incidence of neural tube defects?
Individuals show wide variations in their ability to reduce folic acid (FA). Carriers of certain polymorphisms in genes related to folate metabolism or absorption can better benefit from 5-methylTHF instead of FA. 5-MethylTHF [also known as (6S)-5-methylTHF] is the predominant natural form that is readily available for transport and metabolism. In contrast to FA, 5-methylTHF has no tolerable upper intake level and does not mask vitamin B12 deficiency. Supplementation of the natural form, 5-methylTHF, is a better alternative to supplementation of FA, especially in countries not applying a fortification program. Supplemental 5-methylTHF can effectively improve folate biomarkers in young women in early pregnancy in order to prevent NTDs.
For a moment, let’s move away from how folic acid in utero and see how folic acid affects breast milk.
When looking at how breast milk is affected by synthetic folic acid, one cringes.
“…recent evidence suggests that the somewhat higher affinity of folate binding protein for folic acid than for reduced forms may also decrease the bioavailability of milk folate. . . The markedly lower concentration of milk folate binding proteins compared with prefortification reports along with detectable appearance of unmetabolized folic acid in the milk of even unsupplemented mothers emphasizes the ongoing need to evaluate the potential benefits and risks of long-term consumption of folic acid-fortified foods.”
This means that synthetic folic acid reduces the production of folate binding protein. If folate binding proteins are reduced, then the reduced folates are not getting delivered to the breast fed baby. If the baby is not getting adequate reduced folates, then their methylation and DNA production is negatively affected.
Again, autism is on the rise and so are food allergies – not to mention other neurological disorders and mental/emotional issues. Tough to have a healthy baby with decreased amounts of beneficial folate in their body.
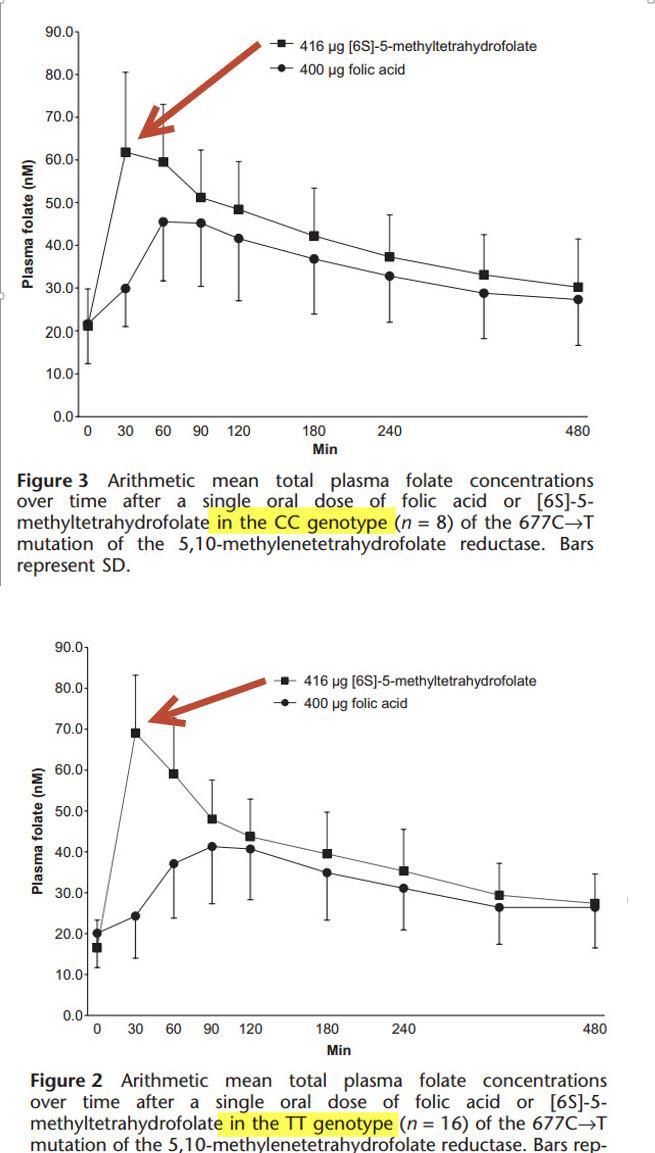
Let’s look at a paper which evaluates how effective folic acid is compared to methylfolate at increasing plasma folate levels. After all, we are looking to increase plasma folate levels in order to reduce birth defects right? There is a plethora of research which associates higher plasma folate levels to decreased rates of birth defects. So let’s look at these two side by side.
The British Journal of Pharmacology published a paper in 2009 entitled, “[6S]-5-methyltetrahydrofolate increases plasma folate more effectively than folic acid in women with the homozygous or wild-type 677C–>T polymorphism of methylenetetrahydrofolate reductase.”
Need I say more?
I’m going to – and I need to.
Note that the researchers only measured ‘plasma folate’. They did not measure intracellular folate. This is important. Can you think of why? Remember that synthetic folic acid binds to folate binding proteins and folate receptors on the cell preferentially over reduced folates like folinic acid and methylfolate?
If this is the case, then we should actually see a decrease in intracellular folate levels in the presence of synthetic folic acid, right?
We do.
That’s bad.
Doctors every day are tricked into thinking their patient’s homocysteine levels are reducing. But what are they checking? They are only checking the blood levels of homocysteine – not intracellular levels nor are they measuring methylation status.
If we want to reduce the incidence of birth defects and optimize the health of unborn children, we need to support one carbon metabolism (aka methylation) in future parents prior to pregnancy. In fact, we really shouldn’t be limiting our attention to folate levels at all – we need to be focused on the bigger picture of what folate actually does – and that is regulate methylation.
Finnell et al say it best: “The effect of one-carbon metabolism on normal neural tube closure extends far beyond just folic acid.”
Then they throw down the gauntlet:
During early embyrogenesis, DNA methylation, which is the chief regulator of gene expression, is epigenetically programmed. Furthermore, it has been well established that methylation of DNA can be influenced by dietary contributions of methyl donors such as choline, folate, and methionine. Any suboptimal methyl-donor supply could alter DNA methylation and provide a ready explanation for a possible mechanism contributing to increase birth defect risk.
Finnell et al. published this in 2010.
It is now 2015.
With the information era exploding with countless ways to access research like this, why aren’t groups like National Birth Defects Prevention Network and the CDC accessing it? I mean, aren’t they wanting to reduce birth defects?
Things evolve.
Folic acid is old hat, out-dated, worn out and needs to go away. And now.
National associations and physicians need to engage, access current research, digest it and implement it.
How did folic acid get into the foods anyhow if it is so bad?
Great question.
Rats and mice are used in research as their genetics and gene function are very similar to ours – as humans. However, there are variations at times.
Folic acid metabolism is one HUGE variation.
You see, in the mouse, their folic acid reducing enzyme, the first one, called dihydrofolate reductase (DHFR) is very adept at reducing folic acid into dihydrofolate.
In humans, we do not have a fast DHFR enzyme and so the folic acid bogs our biochemistry down significantly. As it sits around and waits to get reduced into active folates, it ends up binding to folate binding proteins and folate receptors which prevent active folates from doing so – as described above.
Even mice are negatively affected from folic acid!
A very recent study JUST published came out for this lovely Folic Acid Awareness Week – thank you!
Key findings from this paper state that high dose folic acid, 10x higher than recommended, contributes to MTHFR deficiency and thus liver issues.
Why liver issues?
Because the liver does about 85% of all methylation reactions so it is one of the first organs to get negatively affected.
“We suggest that high folic acid consumption reduces MTHFR protein and activity levels, creating a pseudo-MTHFR deficiency.
This deficiency results in hepatocyte degeneration, suggesting a 2-hit mechanism whereby mutant hepatocytes cannot accommodatethe lipid disturbances and altered membrane integrity arising from changes in phospholipid/lipid metabolism. These preliminary findings may have clinical implications for individuals consuming high dose folic acid supplements, particularly those who are MTHFR deficient.”
Ouch.
Look at all the foods, drinks and supplements which have folic acid in them. Then add up how much folic acid you think you consume in a day. Yes, some people are deficient, but there are also many that are getting way too much.
Folic acid is not what we should be recommending anyway. We should be recommending folinic acid and methylfolate. The days of folic acid should be numbered. It’s an old, archaic ingredient that needs to be tossed. Nutritional biochemistry has evolved significantly. There is no reason to keep using folic acid at all. The only reason to keep using it is because it is inexpensive and companies which use it are making more money off it is due to higher gross margins. Folinic acid is not that expensive. Methylfolate, however, is extremely expensive.
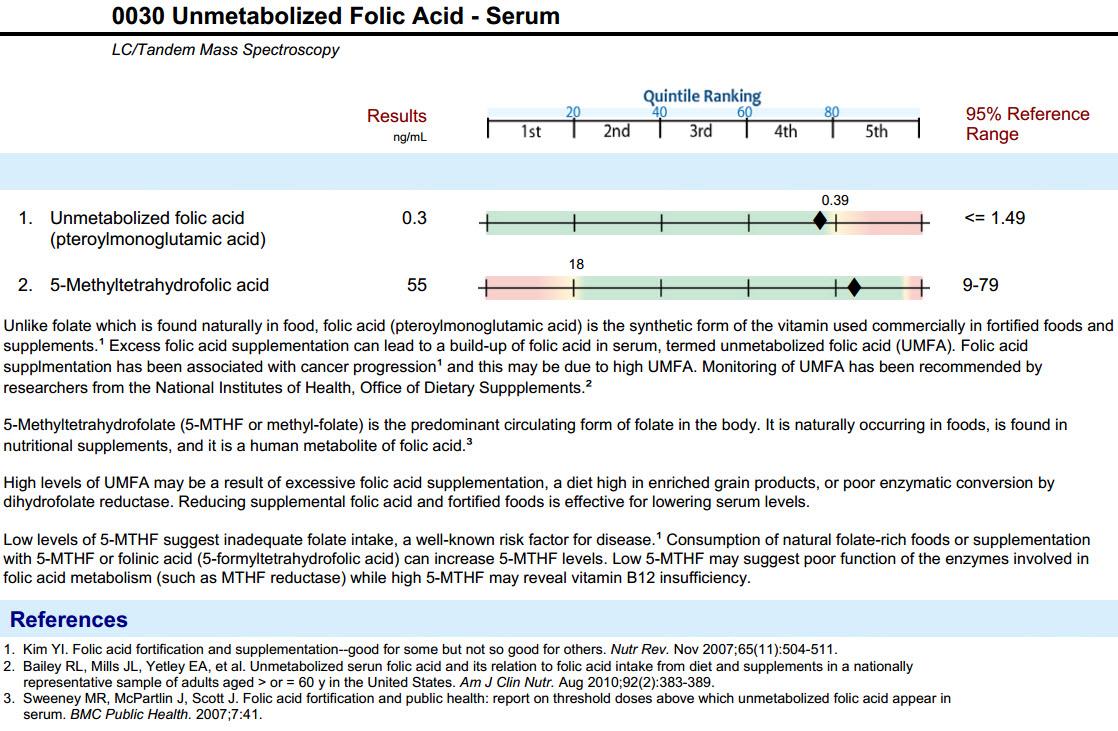
Lab Testing Your Folate Levels: UMFA, Methylfolate and Others
UPDATE: Jan 2015, the UMFA test is no longer available as doctors did not order it enough so the lab discontinued it. This goes to show you that awareness is still very low about the harms of folic acid and UMFA levels.
Some laboratory testing companies are cutting edge and offering UMFA lab testing along with reduced folate testing. Genova is one lab and another is Health Diagnostics. Your doctor can open an account with one or both of these labs and begin identifying your folate levels properly. If you don’t have a doctor or they cannot order it for you for various reasons, you may order the UMFA Test here and the Methylation Profile Test
Here is what the UMFA Lab Result looks like. Note that they show both UMFA and Methylfolate levels.
What to do? Action Steps
- Throw out all folic acid enriched foods. These are processed foods such as cereals, breads, pastas, energy bars, drinks, snacks.
- Throw out all folic acid containing supplements.
- Eat folate rich foods. Note that when I state folate, I mean naturally-occurring folates such as dihydrofolate, folinic acid and methylfolate.
- uncooked leafy greens (more you cook greens, the more folate gets destroyed)
- beef liver (organic, free range)
- various beans such as lentils, pinto, garbanzo, black, navy, kidney and lima.
- Opt for supplements containing active folates. Many quality supplement companies are moving in this direction. Seeking Health is the supplement company I created in order to provide physicians and the general public researched ingredients and effective formulations.
- Test your methylation pathway with your physician and see which forms of folate you are low or high in – then correct it.
- Test your genetics and see where you may have blocks in your folate pathway. Knowing this is useful as you can be proactive in bypassing these blocks with various nutrients, avoiding various medications and increasing certain foods.
- After you test your genetics via 23andMe, then run your raw data through StrateGene.
I encourage you, as an individual looking to optimize your health and possibly your future child’s, to inform your physician, friends and loved ones about the dangers of folic acid – and the benefits of reduced folate such as methylfolate.
Health professional or just want to understand the significance of methylation dysfunction during pregnancy, childhood and adulthood?
Two online courses are now available to learn in DETAIL about the harms of folic acid and in depth education about the importance of methylation – how it is affected and how to restore it.
Maternal and Pediatric Implications due to MTHFR and Methylation Dysfunction – this is an absolute must for pediatricians, OB/GYN, midwives, doulas, nutritionists and those wanting to have children.
Methylation and Clinical Nutrigenomics: Part 1
For those who desire more information but not as in depth as the two courses above, I highly recommend this free video discussing folate metabolism:
I believe that it is possible to reduce the incidence of disease of unborn children – and I will do this one physician and one person at a time.
There is nothing more powerful in preventative medicine than reducing disease in the unborn child.
Thank you
Dr Lynch
PS – Throw away your folic acid enriched foods and supplements. Today. That is your way to celebrate Folic Acid Awareness Week 2014. Spread the word.
PPS – Read how folic acid fortification may be associated with increased rates of autism.
PPPS – Learn about prenatal supplementation
Dr. Lynch,
You have no idea how long I’ve waited for this type of explanation. However, I need more help understanding our situation. I would be so appreciative if you email me so I can explain to see if there is anything I can do to correct the situation.
Thanks!
Jennifer
Dr. Lynch, YOU ROCK. That’s all I can say about this post. 🙂
What happens to the folic acid that is floating around in the blood? Thank you for all you do Dr. Lynch.
Hi Christine –
The folic acid which ‘floats’ around eventually breaks down into reduced folates but it takes time and is dependent upon other nutrients being available and the folate reducing enzymes functioning as they should be.
Folates are also stored in the liver. At any one time, we have anywhere from 30 to 50 mg of folate stored in our liver. Ensuring that your liver function is good is important and making sure you are moving bile out of your gall bladder is also important.
According to one paper, “radiolabeled folic acid to a single female subject and observed substantial catabolism and fecal excretion in folate turnover with an apparent half-life (t1/2) of ∼100 days for the primary folate pool.”
The issue is while the folic acid is floating around, it is also binding to folate binding proteins and folate receptors thereby reducing the binding of active folates.
[…] It is especially important to avoid folic acid, which is the synthetic form of folate, if you and/or your baby has MTHFR gene mutations. This does not mean that you shouldn’t consume folate. Synthetic folic acid cannot be converted properly to methylfolate and blocks the folate receptors in people with MTHFR. Try taking methylfolate instead, as recommended by Dr. Ben Lynch in this article. […]
Dr. Lynch,
THANK YOU! I feel tremendously blessed that I found your website as it has provided me with so much information. Information which I plan to share with my OB/GYN this month at my yearly exam. See, last December (2012) I suffered an early miscarriage in which my doc suspected a MTHFR gene mutation. She was right on the money as my results in Jan. 2013 revealed that I was heterozygous for C677T and A1298C (my paternal grandmother was homozygous for C677T). I had a healthy pregnancy and baby girl in Jan. 2010 and have been unsuccessful at pregnancy since. My husband and I keep trying, although for not much longer as I am turning 35 and he is 36.
My main concern/question is, what prenatal supplements should I take? I saw on your website a whole list of supplements and vitamins to take to support those with the MTHFR mutation, but I just don’t see myself taking all of them. Aside from a miscarriage, I don’t believe I suffer from any other symptoms of MTHFR. Your guidance would be greatly appreciated!
Thank you,
Michelle
Hi Michelle –
It depends on what your doc recommends for you.
The basics for prenatal supplementation are:
– prenatal vitamin
– probiotic
– essential fatty acids of some sort – krill and/or fish oil
– vitamin D
Those are the key nutrients.
This article discusses some prenatal supplementation – ones that I formulated – and recommend.
Do note that the man also has to take prenatal supplements as well prior to conception. It is not all about the woman’s health – research is showing men’s health matters as well.
My best to you both.
How does folinic acid and inability to tolerate it fit into all of this?
I assume it will also be floating around in the blood unable to be used and blocking receptors.
All this genetic testing targets people who ONLY under-methylate, NONE of this is meant for people who over-methylate. I am one of the very few who do not have either main snp (1298 or 677), therefore, I cannot take anything with a methyl donor or it sets off a chain reaction of pure anxiety. I can only take folic acid because it helps to clear out all the extra fee floating methyls.
Please do proper research next time, because this type of article will give some people the wrong impression.
Ophelia –
That is not true. The lab report which offers measuring various forms of folate, SAM/SAH and more helps identify if one is over supporting their methylation cycle – especially if homocysteine is added. Before accusing someone, be sure to evaluate the article more fully. Also – there is only so much one can put into an article. This article is about folic acid – it is not about overmethylation. However, if the lab is ordered as recommended, then overmethylation may be spotted by a skilled physician.
Folic acid is not what one should take to clear out extra methyls. No one should take folic acid. Period. If you are concerned about overmethylation – then take less folate in general and support with niacin. This article goes into some detail on methylfolate side effects.
I would like to thank you for sharing your research and findings. I wish more doctors were familiar with mthfr gene mutations. I was recently diagnosed heterozygous for A1298C mutation. I’ve been suffering from many health problems since the birth of my daughter 16 years ago. It started with severe gall bladder, liver, and pancreas infection due to undiagnosed gallstones. I have fibromyalgia, CFIDS, IBS, and depression. My main concern though is my 16 year old daughter who has been diagnosed homozygous A1298C. What effect are all these folic acid enriched foods going to have on her? She likes to drink Monster which has added B vitamins. Is that harmful to her? Right now I have her taking 1000mcg methylfolate and methyl b12 daily. I cannot find a physician that is familiar with this mutation to treat her. Any advice would be greatly appreciated. I am doing what I can to spread the word to family and friends and refer them to your website. Thank you again and God Bless You.
Hi Dr. Ben,
My daughter, who is 29 wks. along in her pregnancy was just tested for MTHFR and is heterozygous A1298C. I am compound heterozygous for both A1298C & C677T mutations (which is why I told her to be tested). Her blood work also revealed thrombocytopenia (100,000 platelet count) and low RBC, Hgb and HCT. Her OB/GYN just called and is referring her to a hematologist to monitor her.
She is quite anxious now and googled the mutation and came upon your article below:
https://mthfr.net/mthfr-a1298c-mutation-some-information-on-a1298c-mthfr-mutations/2011/11/30/
Our concerns are of course preeclampsia which is listed in this article, and the combo of her low platelets and low RBC, Hgb & HCT are favorable for this. She is not exhibiting HBP or swelling. Also, it sounds as though MTHFR has something to do with folic acid synthesis. Is there anything she should be taking or avoiding?? Very concerned about autism as well, especially since she is having a boy and it is more prevelant.
As some background, although am Heterozygous for C677T & A1298C, I had two normal pregnancies – no miscarriages. I did have ITP in 1996 and had to have an spleenectomy. (Seems strange because that is not enough clotting and MTHFR can cause too much clotting). I also have many symptoms listed in the above referenced article, including Migraine with Aura. Also I have a Type I Arnold Chiari Malformation (had decompression surgery on 10/8/13) which I am not sure is related, but it is a kid of neural tube defect. I also have had a lot of surgeries (Gallbladder & Appendix removed and partial hysterectomy).
Would you suggest genetic testing?
Thank you,
Debbie
Dr. Lynch,
What is the normal range of SAM/SAH ? I mean the minimun ratio to understand if I’m undermethilatior and maximun ratio to understand if I’m overmethilator ?
Thanks
Daniele
Is there a relationship between MTHFR defect (mother, father or child) and sex chromosome trisomies? (XXX, XXY, XYY). Obviously the XYY is related to the paternal contribution. Also, are these kids at increased risk for having the compound heterozygous MTHFR defect? Spina bifida and occulta spina bifida? I know for a fact that the XYY boys have an increased prevalence of autism and Asperger’s. These conditions are often overlooked by OB’s and pediatricians.
Also, can you comment on the TMLHE gene defect (deletion) with is found on the X chromosome and affects the production of carnitine from the amino acids methionine and lysine and may also affect glutathione production? I was reading about this on MSGtruth.org — their home page. These individuals respond to low glutamate diets. Supposedly more boys than girls have autism. But then the fact that XYY has a higher rate of autism may indicate something on the Y chromosome itself also contributes — so autism is likely multi-factorial, perhaps several genes, environmentally triggered.
OH — and one more point. According to research on the Y chromosome, it affects the mitochondria of cells regarding metabolism — so that men and women have different mitochondria production. I can’t remember the specifics. Do you know if this relates to methylation or precisely what the difference is?
Hello Dr. Lynch,
I just ordered quite a few supplements off of Seeking Health. My question pertains to my children. I can’t seem to find a protocol for them on the website anywhere. I have ordered the optimal chewable for my 5 year old son (he has one copy of the A1298C) and the kids optimal for my 10 year old daughter (who has one copy of the C677T) since she can swallow pills.
Are these the only supplements they need? Do these optimal vitamins contain everything? I do have them on a probiotic called Good Belly as well. If you can’t advise children, I’m wondering if you could just tell me what your children are taking? Thank you in advance for the information.
I have MTHFR C677T T/T (homozygous). I asked my MD to test folate and homocysteine.
The Serum Folate test result is 19.9. (I also had it tested in 2008 and it was >20).
My homocysteine (nutritional) was 5.5.
Should I be worried about this high serum folate? What does it mean if anything? The homocysteine level seems safe.
I should probably be able to figure this out from your post but I am sorry I am not sure I fully understand it.
Thank you.
Hi Dr. Lynch,
Thank you for all the work you are doing in this area – it is awesome!
I was just recently diagnosed as homozygous for the C677T after a lifetime of “symptoms” and several years of real problems. I have three children who are all healthier than they should be given the fact that they grew in my body! I plan to get all three tested. My youngest has suffered from seizures – triggered by sleep deprivation, and illness. She also suffered a very bad seizure after our doctor had me start supplementing her with some things that typically help seizure kids – including some B vitamins, magnesium, L-carnitine, etc. I believe that her seizures, if they aren’t caused by bad methylation, they are definitely exacerbated by it. She can’t handle any toxic exposure -( artificial sweetener, chlorine) and her seizure from the supplements occurred right at the point when her body would have been starting to detox.
Who would you recommend I work with – I will go anywhere in the country -to get support for evaluating her and then putting her on a proper supplement program? I would like it to be someone who has specific experience working with seizures if that person is out there!
Thank you for your help!
My 30 year old son had a diagnosis of CHARGE syndrome but he does not fit the diagnosis. (He has some features of Treacher Collins syndrome albiet mild) He has a lot of mid line defects Agenasis of the Corpus Colosum, overlapping bones in his forehead, Choanal Atresia, High Narrow Pallette. He was born from my 5th and last pregnancy, 4 miscarriages (2 blighted ovums) and 2 live births (I lost his twin). My other child has midline defects also (internally). I was pregnant 5 times in 3 years and took Iron and Folic Acid that whole time. All three of us are MTHFR and I have 1 CBS and my son has two and presuming that my other child has CBS also. Am I right in thinking that the excess of Folic Acid would have contributed to my son’s unusual congenital abnormalities ?
My husband also has MTHFR (as well as me) so I’m wondering what kinds of supplements he needs to take. We’ve only had one pregnancy that ended in early miscarriage due to blighted ovum so I assume now that I know we both have MTHFR mutations that may have been the cause and would like to prevent it in case we are blessed with another pregnancy.
MTHFR C677T homozygous (both my husband and I). sorry I left that off.
I feel very confused , I have been diagnosed with MTHFR after 3rd miscarriage and my Doctor prescribed me folic acid high dose of 5mg per day. I have been taking since April and have been told that with future pregnancy I should not have any problem .
I had another 2x miscarriages , in July 2014 and one in Sept. 2014, also I was taking penicillin and Heparin from day one , when we found out I was pregnant.
I was reading in more than one article , to avoid folic acid and use folate…
Shall I stop taking folic acid and start folate only ,or could i take both?
is there anyone in similar situation , I would love to hear their opinion / story.
Also , I have 2 yearl old girl already and had absolutely fantastic pregnancy with her, got pregnant 1st time and carry full term without any conplications.
Have you had your thyroid checked and thyroid antibodies?
100 percent of thyroid patients (according to Ben lynch) have mthfr mutation. 90percent have hashimoto…. Both cause miscarriage. If it turns out to be thyroid, start your journey with Stop the thyroid madness. But I’d take folate and eat leafy greens over folic acid for sure.
Dr. Lynch thank you so much for all you do!
I am homozygous A1298C & have had 5 miscarriages. All my tests come back normal? The doctors don’t know how to help me and I can’t find anyone educated about MTHFR. I found your supplements and started them 2 days ago. I know that you can’t prescribe with limited data, but if you could make some medical protocol suggestions I would be grateful. There is less data available for A1298C and I am finding it difficult. I have also tested positive for ACE although I am not sure which SNP I should be reviewing.
Keep fighting for us and our babies! Thank you!
This is so similar to the reverse T3 using up the T3 receptors.. Thanks Doc, you rock.
Dr. Lynch,
You mentioned in your response to someone that her husband should also take prenatals. I’m planning on starting the optimal prenatal vitamin, am I understanding correctly that it’s okay for my husband to take them as well?
Hello Kelly –
Yes, that is correct.
We also have the Optimal Prenatal Protein Powder – vanilla or chocolate. I personally use the vanilla flavor about 3 times a week mixed with frozen blueberries, fish oil, chia seeds, hemp seeds and almond and/or rice milk.
Hello Dr Lynch,
Great read! Very, very interesting. I am histamine intolerant and appear to have my diet under control since the last few weeks. But I wanted to take pre-natal folic acid and indeed my gynecologist prescribed me a box. But now I see I should be taking active methylfolate. Could you recommend a brand that will not interfere with my low histamine diet, low gluten diet? I am based in Eurpe and want to start trying for a healthy baby soon.
Thanks in advance.
Laila
Thank you Dr Lynch,
One question: on the 23andme site I just read about general genetic testing to find out about your ancestry. Does that standard kit include the testing of the folate pathway blocks?
Thanks
Rob
Yes. A number of them.
Dr. Lynch,
Thank you so much for this information! We lost our first child to a chromosomal defect (T13) and are trying to conceive #2. I have been researching prenatals for days, and looked up some of the ones you recommend (although it’s interesting that some of the brands that have folate in their multi put folic acid in the prenatal – like Pure Encapsulations!). What do you think of the New Chapter Prenatal (very popular, carried at grocers etc). It has folate on the label, and when I called to inquire, they told me that they start with folic acid and have some probiotic process that turns it into folate. Does this sound false to you? I like that it is a whole foods vitamin unlike some of the others discussed here.
Thank you!!!!
Jenny
ps. The Seeking Health Prenatal one looks great but it’s $70 for a one month supply. Very expensive!
I am 1298 homozygous. I receive monthly b12 shots from my doctor. Could you list specific supplements I should be taking? I get overwhelmed by all of the choices. My Dr. Just toldme to take a sublingual B12, folic acid, and a baby aspirin.
What about taking folic acid with B12. Im B12 deficiency and take injections every other week and daily B12 pill with folic acid pill .
folic acid should be avoided.
[…] https://mthfr.net/folic-acid-awareness-week-2014-want-awareness-here-you-go/2014/01/08/ NTD prevention with bioactive folate forms […]
If my child (5 years old) is showing symptoms of an MTHFR mutation, should I test myself or the child first?
When should you start consuming folate before getting pregnant… is there a big difference if you don’t consume folate before getting pregnant… I have the Thorne Research 5-MTHF and Thorne Research Basic Prenatal….. I have done 2 miscarriges is the last year
Hi Dr Ben,
I found out I was compound heterozygous after a miscarriage and concieved quickly again the next month but had only just started taking methylguard and a prenatal with folinic acid. I’m currently 10.5 weeks and am so worried about birth defects as I wasn’t/ didn’t have folate in my body. Does this give me a higher chance now of having a baby with birth defects? I’ve got my 12 weeks scan booked but am so worried.
Dr Lynch,
Any comments on this study?
Homocysteine Lowering by Folate-Rich Diet or Pharmacological Supplementations in Subjects with Moderate Hyperhomocysteinemia: http://www.mdpi.com/2072-6643/5/5/1531/pdf
Abstract: To compare the efficacy of a diet rich in natural folate and of two different folic acid supplementation protocols in subjects with “moderate” hyperhomocysteinemia, also taking into account C677T polymorphism of 5,10-methylenetetrahydrofolate reductase (MTHFR) gene. Subjects/Methods: We performed a 13 week open, randomized, double blind clinical trial on 149 free living persons with mild hyperhomocyteinemia, with daily 200 μg from a natural folate-rich diet, 200 μg [6S]5-methyltetrahydrofolate (5-MTHF), 200 μg folic acid or placebo. Participants were stratified according to their MTHFR genotype. Results: Homocysteine (Hcy) levels were reduced after folate enriched diet, 5-MTHF or folic acid supplementation respectively by 20.1% (p < 0.002), 19.4% (p < 0.001) and 21.9% (p < 0.001), as compared to baseline levels and significantly as compared to placebo (p < 0.001, p < 0.002 and p < 0.001, respectively for enriched diet, 5-MTHF and folic acid). After this enriched diet and the folic acid supplementation, Hcy in both genotype groups decreased approximately to the same level, with higher percentage decreases observed for the TT group because of their higher pre-treatment value. Similar results were not seen by genotype for 5-MTHF. A significant increase in RBC folate concentration was observed after folic acid and natural folate-rich food supplementations, as compared to placebo. Conclusions: Supplementation with natural folate-rich foods, folic acid and 5-MTHF reached a similar reduction in Hcy concentrations.
Thanks.
They did not look at intracellular homocysteine – only extracellular. The good researchers are looking at what happens to intracellular homocysteine post-folate or folic acid supplementation. Folic acid lowers homocysteine outside the cell – in the blood – but not inside the cell – which is where it really matters. There are studies which back this up – and I discuss them in this course: Methylation and Clinical Nutrigenomics Part 1
Is it ever possible to rid the body of the synthetic folate floating around in it? If so, what helps with that? We feel a great benefit from using liposomal vitamin C, but I know it may be completely irrelevant to this problem.
I feel very confused , I have been diagnosed with MTHFR after 3rd miscarriage and my Doctor prescribed me folic acid high dose of 5mg per day. I have been taking since April and have been told that with future pregnancy I should not have any problem .
I had another 2x miscarriages , in July 2014 and one in Sept. 2014, also I was taking penicillin and Heparin from day one , when we found out I was pregnant.
I was reading in more than one article , to avoid folic acid and use folate…
Shall I stop taking folic acid and start folate only ,or could i take both?
is there anyone in similar situation , I would love to hear their opinion / story.
Also , I have 2 yearl old girl already and had absolutely fantastic pregnancy with her, got pregnant 1st time and carry full term without any conplications.
[…] can you do fix the epigenetic epidemic? That’s another blog post, but to start, eat folate, not folic acid. If you’re a woman on hormonal birth control, stop taking it. Don’t use antacids. Go […]
Thanks for the article. I’m taking an active dose of folic acid with Quatefolic. Is it folic acid all together that should be avoided or is the active supplement ok? Thanks.
Folic acid needs to be avoided.
Dr Ben,
You mention near the start of the article that folic acid fortification appears to have reduced the incidence of neural tube defects. Are you saying this would only be possible in people who don’t have an MTHFR polymorphism? I was on 5mg of folic acid on top of what was in my prenatal multi, due to a family history of NTD, and I have the homozygous c677t mutation. Somehow my daughter doesn’t have a NTD and I am wondering if taking so much folic acid meant I was still able to convert enough of it, even with my reduced enzyme activity, to prevent her having a NDT? It sounds like this is unlikely from what you have said but as this process is complex and the stats show reduction in NTDs with folic acid supplementation, I am unsure. Can you clarify this for me?
I really appreciate this article. I went through my cupboards and found that “folate” is in my Simply Orange not from concentrate OJ. I was glad it said Folate and not Folic Acid; however, is there still an area for concern? Should I trust this is a naturally occurring folate and not a fortified ingredient? Also, do you find that doctors are generally open to reading this research in your article when it’s presented by a patient? I will try to ask my OBGYN to read this and test me but I have my doubts that she’ll be willing. Any advice in this area of persuasion is most appreciated. Thanks for your work.
I suspect that it is added and not natural folate.
This is what the FDA is actually trying to fix by new labeling laws -and I agree.
Companies cannot use the word ‘folate’ when it is actually ‘folic acid’ – but they do.
Is the methylation panel you suggest available for the UK?
If not what would you recommend instead? e.g. Doctor’s data methylation profile?
I have been diagnosed with mthfr homozygous c6771. I want to stop taking folic acid as i know it is bad. Please, can you tell me what shound i take and what dosage? We are trying to conceive again after a miscarriage. Should i take folate or methylfote? Or is this the same thing? Would really appreciate your help. Thank you in advance 🙂
Hello –
Please read this article on prenatal supplementation – will help a lot 😉
https://mthfr.net/prenatal-supplementation-optimizing-your-future-child/2012/01/20/
This is a very interesting argument. I’m curious about my own experiences. I started eating all organic food, eliminating everything with folic acid added, and was in very good health. I got pregnant with my daughter, who was later diagnosed with anencephaly. She died in 2002. Since that time, I was told I had the MTHFR gene mutation, and a geneticist recommended that I take 5mg folic acid, 200 mcg’s of B12, and 100mcg’s of B6. He said they needed to work together to prevent future neural tube defects. I have done this and had 5 healthy pregnancies. I am very nervous not to take folic acid and my other vitamins daily, because when I did as you described above, I had a baby that died. I’ve also read so many studies about the positive reduction in neural tube defects from synthetic folic acid supplementation. What do you recommend for someone in my position?
Kellie –
I recommend using folate – that’s the key – not folic acid.
Folic acid is a synthetic form of folate. You want the natural body preferred forms -which are folinic acid and methylfolate.
Dr. Lynch,
I’m a little confused by the chart above. Does folinic acid require b6 or b2 in order to be converted to methylfolate?
A link to this article has been sent to the good folks at Meyenberg, because they add folic acid to their powdered and canned goat milk (the carton milk is ok). In their words:
“We currently add folic acid to our Evaporated and Powdered products since the USDA has specific recommendation on folic acid needs when consumed by younger children. Since goat milk is naturally lower in folic acid than cow’s milk we do fortify some of our products with the folic acid for this reason.”
We need to educate and put pressure on our food manufacturers to stop adding folic acid to their products. I encourage anyone who buys Meyenberg goat milk to write to them at info@meyenberg.com and encourage them to switch to folate instead.
Hi Dr Lynch,
Thanks for this great explanation. I am wondering whether I need to invest the money and time to go down the route you suggest with all the lab tests.
I have always had overly high serum folate levels. The tests tended to be done at times when I was supplementing folic acid. I have had 3 babies and the last pregnancy ended in miscarriage (that was the only time when I started supplementing folic acid before pregnancy. The other times I only supplemented once I realised I was pregnant. Not sure if that had a part to play in the miscarriage or perhaps other reasons that happened the year receeding e.g. stress: death in family and digestive issues following food poisoning). I have noticed that each child does have speech delays. My 4 year old still can’t pronounce all her letters and sounds e.g. ‘s’. My 6 yr old can now finally pronounce words well. They seem to be 1 year behind their peers.
Do you think that would be enough to suspect methylation problems?? Is there one test I could do first to help decide if I should do them all?
It’s just that I’ve already spent so much money looking into food sensitivities and gut pathogens but I would like to have another baby in the future…..
Many thanks!
Some of pictures is not displayed.
Any trouble?
I wish I could see the graphics. I want to share this with people who actually NEED the images…I get a 404 error or just place holders for ALL the graphics. TIA. Great work. You rock. Dr Carl.
Hi Dr. Carl – This has been resolved. Thank you for pointing this out.
Hello Dr Lynch
Thankyou so much for your invested valuable knowledge. I found out this week I have Heterozygous C677T/A1298C. I.ve been taking 300 to 400mcg folic acid in iron tablets due to anemia for the last 2 years. My strange health issues started from this point on but I was unaware and so were the GP’s of the gene mutation and obviously the process of synthetic folic acid with MTHFR. I suffered with major menstrual issues for the last 10 years through eating well I felt I was helping my health exercise was a constant enjoyable part of my life. I never needed to see a Dr as I felt healthy never got sick (just menstrual got worse)etc. So 2 years ago anemia is diagnosed iron tablets containing folic acid prescribed. 6months later Currette performed…1year later Ablation..during this time still supplementing with iron folic acid as neither operations worked for my body. During this time I had an unfortunate incident cleaning out my bathroom with a chemical which caused ripping stomach pain for 24hours. A&E sent me away with no testing just saying I could.ve killed myself. My health was deteriorating and so was my life and lifestyle. I was a regular at A&E as I started having allergic reactions and very strange body symptoms. I knew in myself something was not right. As time went on I felt I had enough of feeling Dr’s G.P’s Naturopath’s thought it was in my head as they’d do tests but nothing. In my opinion that’s the KEY….TESTS (the correct tests) weren’t performed. I was reacting to naturopath tonics prescribed. I stopped going to the Dr’s and suffered silently at home. My work has suffered everything in my life has suffered as these strange reoccurring symptoms contiued. A friend guide’s me to a Chiropractor by this stage I don’t have faith in anyone to help me it’s over for me. After weeks of pain and hesitation I pluck up the courage and go. A Holistic Chiropractor I explain my symptoms he acknowledges does kinesiology on me and explains the detoxing. I.m so scared by this stage to ingest anything as the reactions I had experienced through pills and tonics are debilitating. So 6weeks later I start to trust again and have the vitamin B6/12 and MTHFR drops and I feel no major side
effects…I.m still taking the folic acid iron tablets all this time…I start to feel good but my iron still not increasing and menstrual out of control..my Chiropractor leaves town but orders me MTHFR blood tests August 2015. I start to feel off again. I received my results to my test this week January 2016 advising of the mutation. (Long story). I had a hysterectomy September 2015. I.m off the vitamins B6/12 and MTHFR and just taking folic acid iron tablets again. My iron still low advised by a naturopath to take 4 iron tablets in one day and then nothing for four days to help my body store iron. Well I froze I said with my history I don’t feel it is right but I.m desperate to feel better and increase this iron that won’t improve. I attempt it slowly 2 iron tablets in one day 12 hours apart 2 days with no iron tablets it seemed ok…2weeks later I try to have 3 folic acid iron tablets…by the 2nd tablet I was non conherent I felt like a blob I was unable to function I felt I was going into a black whole and pass out. This was November 2015 since then I.m back to my crazy symptoms I now get sick eating food my gut feels off I have sharp stabing pain all over. Was advised by my G.P. 3 weeks ago I.d poisoned myself wait a week and then have another iron tablet. So I wait a week and end up with the same terrifying ongoing symptoms that haven’t stopped. I am no longer taking the iron tablets. I am suffering worse than ever now with food reacting instantly. Last Tuesday I got my MTHFR results from my Chiropractor and started researching myself. All I can say is if I had.ve got these results 6 months ago I would.nt be where I am today. I rang my old Chiropractor yesterday and he was shocked I only received them now. I am grateful I have them but my health is alarmingly not good. I am feeling the effects of the rampant folic acid In my blood making me ill. I am so very scared to go to hospital as they have never helped. I am off to the Chiropractor in the morning for help. I gave my G.P the test on Wednesday unfortunately her knowledge is limited in this field.
Thankyou for your valuable knowledge and guidance.
Lorraine
Hello –
After two miscarriages, I’ve found out through genetic testing that I’m heterozygous MTHFR-A and heterozygous Factor V Leiden. My doctor has prescribed me to be on 4mg of folic acid daily, for which I was prescribed daily: Folgard, 2 800mcg tabs of folic acid, and Women’s One a Day + DHA. I’m also on baby aspirin. I’ve read so many conflicting articles that I don’t know what I need to be on! Any info helps 🙂
Justine –
This article has helped many women – I highly recommend considering what is here – and working with a health professional who understands why folic acid is not the right choice –
This article may help you a ton –
https://mthfr.net/prenatal-supplementation-optimizing-your-future-child/2012/01/20/
Woman’s One a Day is NOT going to suffice – not even close –
Please do consider strongly the Optimal Prenatal – either as capsules or as the prenatal protein powder (as a smoothie in the morning 😉 ). This formulation took me about 3 yrs to formulate – after much research.
I’m not sure anyone is answering questions here but is folinic form (no methyls) ok? I can’t do methyls and will not try even at small doses. Thanks!
Folinic can be slowly converted to methylfolate in most people. But it is the form of folate found in food so it should not be a problem.
Thanks! All folic forms eventually turn into methyl form, right? I purchased the folinic seeking health form and hopefully that coverts the same as the prescribed folic but without the damaging potential to the binding protein that synthetic access could cause. And not induce over methylatibg myself since I have breakdowns there. I know the dr has me avoiding methyl foods but perhaps it’s a balancing act of how much how fast…
Thank you for the reply
I wouldn’t worry about it at all. Again, it’s the same folate as found in foods, and there’s folate in almost every food group. If you had a problem you would starve to death.
Not sure what your doc means by “methyl foods”. The protein used in methylation is methionine, again, in almost every food, but to my knowledge there are no specific methyl-foods. I’d ask him what they are, and then please list what he says here.
Doesn’t make sense to me.
Thanks! Yes I think it’s about not tipping the scales until my methylation jams are corrected. Something about my methionine being high and recycling/not being converted so temporarily have to be careful with methyls (avoiding adding more) and some foods are much higher than others in the chemical breakdowns to methyls. It’s a sea-saw balance!
I recently took many blood tests after two miscarriages in a row. Everything came back normal,however, my doctor told me that I’m slightly low in the enzyme MTHFR. My doctor told me that it isn’t necessarily the cause of my miscarriages, but could possibly be. As a result, she is me on 5mg of folic acid as well as a prenatal vitamin. I’m so confused with all of the information? Since I’m only “slightly low” is taking 5mg of folic acid helpful or harmful? Please help.
5 mg of folic acid is the standard of care for recurrent miscarriage.
I don’t agree with this recommendation.
This is what many have read and used:
https://mthfr.net/prenatal-supplementation-optimizing-your-future-child/2012/01/20/
Have you tested for Factor V Leiden? It’s a clotting disorder.
This is why we all should avoid folic acid – I dig into the science and explain it in easy vocabulary:
https://www.youtube.com/watch?v=cWFPRI6X7P4